|
Author
|
Topic: Exam for discussion
|
Bob
Member
|
 posted 05-23-2008 11:47 PM
posted 05-23-2008 11:47 PM
 
After some experimenting with transfer and edits- These charts are being posted because I thought they would be of interest and possibly fuel some discussion. Case Hx: The subject is a 54-year-old male hispanic who engaged in inappropriate sexual behavior with his 4-year-old grand-daughter. The subject has been in counseling for two years and has undergone multiple polygraph examinations. Med. Hx: The subject reports his current general physical health as “Good.” He reports no current medical concerns of significance relating to his neurological, cardiovascular, respiratory, musculoskeletal, or gastrointestinal systems. He has a common visual anomaly requiring visual acuity correction; he does not report any auditory deficiencies. He states he is not a user of tobacco products. He reports the current use of a prescribed or over-the-counter medications:
Abilify 10mg
Depakote 1000 mg Cht 1a
 Cht 1b
 Cht 1c
 Cht 2a
 Cht 2b
 Cht 2c
 Cht 3a
 Cht 3b
 Cht 3c
 Cht 4a
 Cht 4b
 Cht 4c
 Cht 4d

[This message has been edited by Bob (edited 05-24-2008).]
[This message has been edited by Bob (edited 05-24-2008).] [This message has been edited by Bob (edited 05-24-2008).] [This message has been edited by Bob (edited 05-24-2008).] [This message has been edited by Bob (edited 05-24-2008).] IP: Logged |
rnelson
Member
|
posted 05-24-2008 02:22 PM

Abilify + Depakote...Depakote was original an anticonvulsant for seizure disorders, but has proven useful for mood instability (bipolar disorder), intermittent explosive disorder, and other aggitation/anger problem and emotional lability. Abilify is a neuroleptic. Long term Depakote may contribute to some cognitive decline, so a lot of docs are increasingly reluctant to use it unless necessary. Abilify is sedating. That is often regarded as a side effect, but its used strategically to help settle down intractable folks. Your guy may have a stubborn and disruptive bipolar disorder. quote:
He has a common visual anomaly requiring visual acuity correction
= wears glasses C6 is too early to use on chart 1 and there is mvt at C9, making R10 uscorable. The P02 sensor data is suspicious looking at C6 on chart 2, but not much shows through the motion sensor. There is abdominal activity at the point of answer throughout the test, and it seems to become more and more prominent across each chart. Looks like a ZCT to me. Blocking at answer on R5 on chart 3. Aside from that, after three charts I have: R5 = +1
R7 = -8
R10 = -4 DI This is scoring three position only, quick and dirty,right from the screen. With the fourth chart, I've got, R5 = -1
R7 = -6
R10 = -6 The pneumos are quite desynchronized on charts 2 and 4. That looks suspicious for a lot of conscious attention to his breathing. Can you tell us the purpose, or the targets, and questions? r ------------------
"Gentlemen, you can't fight in here. This is the war room."
--(Stanley Kubrick/Peter Sellers - Dr. Strangelove, 1964)
IP: Logged |
Fed Employee
Member
|
posted 05-24-2008 10:20 PM
I have a DI to R7. ZCT?My issue are the pneumos - inconsistent. Attempted countermeasure? IP: Logged |
rnelson
Member
|
posted 05-25-2008 12:29 AM
quote:
Case Hx: The subject is a 54-year-old male hispanic who engaged in inappropriate sexual behavior with his 4-year-old grand-daughter. The subject has been in counseling for two years and has undergone multiple polygraph examinations.
for the sake of discussion... grandparents don't sometimes engage in "inappropriate sexual behavior" with their 4 year-old granddaughters (which begs the questions, what kind of sexual behavior would be appropriate). Some grandparents unfortunately do "sexually assault" their grandchildren. Also, one would hope this gentleman had participated in two years of "sex offender treatment," not "counseling." Sex offender treatment is very different from "counseling." Sex offender treatment is more directive, more intrusive, and less confidential. Counseling is supportive, warm-fuzzy, empathic stuff. Sex offender treatment is focused on learning to manage one's abusive behavior, and that means taking responsibility for the behavior, the precursors or warning signs (and we hope there are warning signs else you have a very dangerous offender), and planfulness (and we hope there was some planning, else you have a dangerously impulsive dude). Sex offender treatment is about deviancy. Offender sometimes want to desexualize their offenses. That is fine, if it is accurate. But keep in mind that people who sexually can assault other without sexual arousal are probably much more dangerous than others. Offenders often want to say they go to "classes." It's always fun to play dumb and ask about what kind of classes they go to in addition their sex offender treatment. I'm mostly interested in their treatment, but the classes are interesting also, so I want to know about that too... but lets start by telling me all about the treatment first. Offender's prefer to portray their assaults as "inappropriate touching." In fact, most know their behavior would be considered egregious, else they wouldn't hide it from others. They will also tend to give their victim's present age - if they wait long enough, their victims become adults, and it doesn't even sound like an assault anymore. In this case, its important the victim was age 4. Part of the victim and family impact will be the that normalcy and trust is shattered. Some families' desire for normalcy motivates them to deny ongoing risk, which, of course, increases ongoing risk. The alternative is to live in a family context that becomes overshadowed with concern about sexual risk (what's an offender to do). So, just how distorted, self absorbed, and absent of internal boundaries would a grandparent have to be to allow oneself to become sexually aroused to a 4 year-old granddaughter??? Also, what would an authentically conscientious offender do under the circumstances. My guess would be that if an offender actually allowed himself to experience actual feelings about that, he'd feel like a bucket of puss and become maybe become a little suicidal. So, its not surprising they chose the fake/mask route of ego management - and say disgusting things like "inappropriate sexual behavior" with a 4 year old granddaughter," instead of "sexually assaulted."
.02
r
------------------
"Gentlemen, you can't fight in here. This is the war room."
--(Stanley Kubrick/Peter Sellers - Dr. Strangelove, 1964)
IP: Logged |
Bill2E
Member
|
posted 05-25-2008 08:39 AM
Abilify 10mg
Depakote 1000 mgI first have a problem testing this individual on these medications. I would want a statement regarding why he is on these particular medications. It appears that there are breathing countermeasures present, however this could be due to the medications. R7 shows deception clearly with a -7 overall for me. and I hate the auto centering on the pneumos, makes it more difficult to see the overall picture. (global) Ray, most offenders minimize to the max on their offense and maximize to the max on the victims part of the molest. Would be nice if they would take full responsibility for their actions, however they do not. That is the reason for recidivism. IP: Logged |
rnelson
Member
|
posted 05-25-2008 09:08 AM
Bill,I got it. I'm just ranting. If I've said it once, I've said it a thousand times... 5 year-olds don't "give oral sex." A fact of life is that psychiatric problems are overrepresented among sex offenders and other criminals. What I would do is ask and document is explanation for why he takes those meds. A good "counselor" or "therapist" would have educated him about his mental health disorder, and he should be able to say "I'm better with those meds." He should also know the name of his psychiatrist, and meds like this should not be administered by a family doc or GP. If he doesn't know why he takes these meds, then the therapist should be alerted. Ask if he experiences any troublesome side effects - like falling asleep while operating heavy equipment. Can he work? Can he drive? If so, and absent any side effects or titration problems, then he can probably take a polygraph just fine. People who function optimally on meds, will most likely produce polygraph data of optimal interpretable quality while on their meds. Never tell someone not to take their meds. An important thing to note, is that this combination of meds appears intended to take the edge of a manic or otherwise intractible (probably bipolar) disorder, which does sometimes include psychoticism (loss of reality contact). Bipolar people also sometimes self medicate with excessive use illegal drugs and alcohol, so excavating the history may actually be difficult. Still, most offenders do recall what they have done and to whom they have done it, and that is what matters. I agree though, Bill, that this guy is arguably NOT a normal functioning person. He probably presents a very different picture when he's not on meds. This is, of course, only important only if you are interested in a scientific approach to polygraph validity - which means statistical classifiers based on normative data. His breathing stinks, but he's DI. I'm not sure what you are looking for with overall or global picture. What are people's current thoughts on reporting DI when we suspect someone may be intentionally distorting their data? r 
------------------
"Gentlemen, you can't fight in here. This is the war room."
--(Stanley Kubrick/Peter Sellers - Dr. Strangelove, 1964)
IP: Logged |
Bob
Member
|
posted 05-25-2008 12:18 PM
Good Morning all-Additional Case information: The subject has been participating in Sex Offender Treatment (with the inclusion of weekly group sessions), he also attends an S.A.A. program as well. Sexual Hx disclosed to date: as an adult [>18] one 4-year-old female victim and two 15-year-olds. Although at age 9, he reports sexual behavior with two family females (ages 6 and 4). Other historical paraphiliac interests or behaviors included: voyeurism, exhibitionsim, fetishes, olfactophilia, somnophilia, zoophilia. He admits he has sexual interest in pre-adolescent female children and visualizes seeing them nude. [I see him as a fixated pedophile and therefore, yes, dangerous. However I am no therapist.] His Hx includes multiple age appropriate sexual contacts, and has been married 3x. He has taken several exams addressing whether or not he reported all sexual contact with minors. None of which he has ‘passed.’ He ‘alleges’ the test failures are due to his extreme shame and guilt over the molestation of his grand-daughter, and his sexual interest/ fantasies of pre-adolescent females; and not that other victims exist.
The offender’s family wanted him to attend [then] upcoming family gatherings over holidays [where of course children were going to be present]. He prepared a protection plan which was approved, and authorization to attend was dependant on ‘passing’ an exam over Sx Hx issues. In effect, the therapist was utilizing the re-test as a ‘carrot’ to ‘cough it up’ in order to attend. The purpose for posting these charts (which I deliberately chose not to state in advance) is exactly what Ray is now posing as a question quote:
What are people's current thoughts on reporting DI when we suspect someone may be intentionally distorting their data?
Dr Barland and I recently had an email discussion on this topic (but not about the presented case). However, I first wanted to see how other examiners would interpret the data (DI/ NDI/ NO); and then present my decision and the Examinees post test statements; in the end -as Paul Harvey would say ‘You [will] now know the rest of the story’.Ray commented quote:
grandparents don't sometimes engage in "inappropriate sexual behavior" with their 4 year-old granddaughters (which begs the questions, what kind of sexual behavior would be appropriate). Some grandparents unfortunately do "sexually assault" their grandchildren
No argument. The verbage “inappropriate sexual behavior” are my descriptive words and not the offenders. Ray said quote:
My guess would be that if an offender actually allowed himself to experience actual feelings about that, he'd feel like a bucket of puss and become maybe become a little suicidal
. He does [if you want to believe him, that is] and is the reason for the meds. Ray: quote:
...that this guy is arguably NOT a normal functioning person. He probably presents a very different picture when he's not on meds.
I have met with this client before taking the meds, and after the meds, frankly I do not see any difference in his behavior or the way he presents himself. He self reports however his feelings of being on an ‘emotional roller coaster’ as subsided. Bill2E: quote:
I hate the auto centering on the pneumos, makes it more difficult to see the overall picture
These are not auto centering pneumos. The EDA recording is being recorded in both manual and detrended modes however. Bob [This message has been edited by Bob (edited 05-25-2008).] IP: Logged |
rnelson
Member
|
posted 05-25-2008 04:49 PM
Thanks Bob for the Paul-Harvey, and for the interesting case. quote:
Good Morning all-
Additional Case information: The subject has been participating in Sex Offender Treatment (with the inclusion of weekly group sessions), he also attends an S.A.A. program as well.
His SAA program may be ill-equipped to comprehend and respond to his pedophilia. They probably don't actually know he's a pedophile. (Would they support his attendance at a family reunion with lots of kids if they knew?)
quote:
Sexual Hx disclosed to date: as an adult [>18] one 4-year-old female victim and two 15-year-olds. Although at age 9, he reports sexual behavior with two family females (ages 6 and 4). Other historical paraphiliac interests or behaviors included: voyeurism, exhibitionsim, fetishes, olfactophilia, somnophilia, zoophilia.
There is a tendency for professionals to over-utilize labels in communicating these things, and under-utilize a description of the behavior or issue. Diagnostically, “paraphilia” means “causes distress is social, occupational or interpersonal functioning” There is a lot that sex offender therapists might want to know about, which does not qualify as a paraphilia. Its history. Some of it is important, some unimportant. Sex offender therapists have not always exercised ballanced professional judgment around things. For example, I still hear from some offenders that they are taught that it is deviant (masturbatory deviancy) to masturbate to thoughts or fantasies of anyone unless you have obtained their permission first. “Deviant,” by definition, mean way outside normal limits – things that are so weird or wrong that we don't want them occuring in our neighborhood, even if behind closed doors. (A rule of thumb is: if it's OK as long as it's behind closed doors, then its probably not “deviant” in a diagnostic sense.) Is his voyeurism history as a juvenile or as an adult? How persistent across his lifespan? Are there periods of abstention? Why? Here, some frequency and description is helpful to assure a reader that we're not talking about juvenile behavior, college pranks (mooning/tea-bagging), or household nudity. What about his exhibitionism? I've heard therapists tell a treatment group that peeing in the woods or in a cornfield late a night is exhibitionism. It is not. Exhibitionism would be peeing on a street in broad daylight where everybody can see all your bidness. Exhibitionism can be the loose/bagging clothign “accidental” exposure type, or the deliberate household nudity in front of underage relatives type, but mostly involves intentionally exposing oneself in public. Fetishes is too broad a term to convey anything useful. Olfactophilia. So, he's aroused to perfume, or does he sniff soiled underwear or undergarments? How persistently across his lifespan. If its been ongoing since childhood that tells us something. If this has emerged as an adult, that tells us something else about the plasticity of his deviancy Somnophilia: some description would help us understand whether you mean waking his wives up at night, or sneaking into his victim's bedrooms. Or, sexual contact with intoxicated/unconscious persons. Some lifespan detail would be helpful. Zoophilia: He's hispanic. Is he an immigrant? I've hardly met any immigrants from rural Mexico who had not engaged in sexual contact with animals. What would tell us more is some lifespan/age information, and whether the behavior persisted as an adult (or after moving to the US, where cultural tolerance may be different) Not suggesting that Mexico condones this, but it may not hold the same signal value for deviancy in some subcultures. Peristence after immigration is more diagnostic of a person who does not conform well to norms. quote:
He admits he has sexual interest in pre-adolescent female children and visualizes seeing them nude. [I see him as a fixated pedophile and therefore, yes, dangerous. However I am no therapist.] Non-fixated pedophiles can be dangerous too. BTW, the term “fixated pedophile” is outdated. Years ago, we used to think of pedophiles as either “fixated” or “regressed.” Current DSM-IV TR codes include “exclusive” and “non-exclusive” subtypes for pedohilia. Exclusive means someone is aroused only to prepubescent children. That does not seem to be what you describe here. [quote]His Hx includes multiple age appropriate sexual contacts, and has been married 3x. He has taken several exams addressing whether or not he reported all sexual contact with minors. None of which he has ‘passed.’ He ‘alleges’ the test failures are due to his extreme shame and guilt over the molestation of his grand-daughter, and his sexual interest/ fantasies of pre-adolescent females; and not that other victims exist.
Here you can see his labeling tendency, in the words “victims exist.” Victims a both a label and jargon. Of real concern is whether he sexually assaulted other children – not whether other children exist, and not whether they are “victims” in an existential sense. Behavior, not labels. (repeat: behavior, not labels). What if those “victims” don't know they are victims ('cause they were asleep or unconscious), or don't want to be called victims (I've met adolescent male victims who would punch you in the face if you called them a victim – some victims used to want to be called “survivors,” but that is now becoming a bit trite). The point is that we are interested in the behavior, not the label, and not someone else's state of existence or categorical status. What did he do, and to whom did he do it? Things like this will help us to be perceived as more credible by other professionals. Married 3x does not suggest a pattern of exclusive type pedophilia. The sex history target “reported all sexual contact with minors” may be part of the problem. This is ambiguous in that it seems to address the issues of 1) sexual contact with other minors, and 2) the number and types of assaults against those minors. There is always more. Only a damn fool would think he knows everything these offenders have done to their victims (and it's a disservice to victims to make that assumption). He might be minimizing the number or invasiveness of the instant offense. Are the details of discrepancy in the allegation and his version? You can see a bit of ambiguity and caginess in that the assault involves/implies arousal, while shame and guilt for most people are inversely correlated with arousal. So, which is it? Arousal to children, or ashamed? Or is this another paraphilia, in which shame itself is arousing? He's probably just not being completely straight, and has learned to tell others what he thinks they'll find acceptable. quote:
The offender’s family wanted him to attend [then] upcoming family gatherings over holidays [where of course children were going to be present]. He prepared a protection plan which was approved, and authorization to attend was dependant on ‘passing’ an exam over Sx Hx issues.
Question: So what would a really good protection plan look like, from a family that appreciated the threat this “pedophile” presents to the children? Answer: “we'll save you some ribs and some ice-cream for later” (they would ask him not to attend – that they want him to attend, seems to suggest they don't get it and may not be capable of protection) Here's the joke: he'll be safe to be around his family members when they decide he's not safe to be around them. Only its not funny. There's no magic-therapy wand, or magic-therapy-dust to make this all better. This is a humpty-dumpty type problem. He sexually assaulted his granddaughter, and now wants to be “trusted” around other children. Access to those other children in the past may well be part of what is missing from his reported sexual history. quote:
In effect, the therapist was utilizing the re-test as a ‘carrot’ to ‘cough it up’ in order to attend.
Lemme get this straight. He's an admitted sex addict. You think he's a pedophile and they want to send him to family activities with children??? Try this: Mr. Crack Addict, for doing a good job admitting your crack-addiction, we're going to let you spend the holidays at the crack-house.... Some therapists do things hoping it will work, without really knowing what they are doing. They also tend to over-rely on the jack-ass theory of motivation. (aside: all motivation theories falls into three categories 1) jack-ass, 2) marine corps, and 3) godfather) quote:
He does [if you want to believe him, that is] and is the reason for the meds. Ray:
OK. Abilify is used for these intractible lability problems, including managing thoughts of self-harm. quote:
I have met with this client before taking the meds, and after the meds, frankly I do not see any difference in his behavior or the way he presents himself. He self reports however his feelings of being on an ‘emotional roller coaster’ as subsided.
Not surprising. Most people are on good-behavior at their polygraph. They can be much more unreasonable and much less cooperative with others.
Enough for now. I'm hoping to be home before midnight.
.02
------------------
"Gentlemen, you can't fight in here. This is the war room."
--(Stanley Kubrick/Peter Sellers - Dr. Strangelove, 1964)
IP: Logged |
Bob
Member
|
posted 05-26-2008 01:13 AM
Good Morning Ray and Everyone- The main purpose of my post is the analysis of the polygrams- I just presumed the readers of the forum would like a little Case Hx, and in particular the Med Hx/drugs which could impact the polygrams. The extent of the sexual history, and the test questions posed primarily are irrelevant (now don’t jump down my throat- about the test questions being irrelevant, I throughly understand poor test question construction is critical to a test). The main interest here is ‘what do-ya see in the charts’?; Are countermeasures being employed? If we come to a decision that countermeaures are being used, what studies (if any) can be utilized to support that decision (absent an outright blatant admission by the examinee)? If the data is physiologically or medically ‘abnormal’ (excluding a medical cause), then it must be intentional- and if it is intentional, then it must be a countermeasure? In a previous post “Unscientific Training”,Ray reported that Nate Gordon provided a presentation at a conference wherein he said quote:
Pulse/respiration ratios that are significantly different from 4:1 are a countermeasure signature
which by the way I tend to agree- but that is another topic. If we cannot support a countermeasure decision, how should we report it and what impact should it have in our final analysis? Which goes right back to Ray’s question quote:
What are people's current thoughts on reporting DI when we suspect someone may be intentionally distorting their data?
I’ll add- “or NDI”Please bear in mind everybody that the words being used in writing a brief of the case facts are my own phrasing and ‘labels’ (i.e. victims) and should not be construed as a quotation from the offender. As Ray pointed out, and I do not disagree quote:
Diagnostically, “paraphilia” means “causes distress is social, occupational or interpersonal functioning” ....There is a lot that sex offender therapists might want to know about, which does not qualify as a paraphilia. Its history. Some of it is important, some unimportant
although from my perspective- if a person were to tell me they have a sexual interest in, frequent fantasies about, or behaviors in doing- it qualifies; the therapist can determine if it “causes distress in social, occupational or interpersonal functioning” or has reached a ‘deviate’ level. On your ‘aside note’ Ray “ all motivation theories falls into three categories 1) jack-ass, 2) marine corps, and 3) godfather”; I presume you are referring to the Corps motivational theory of ‘kicking your ass’? Bob
[This message has been edited by Bob (edited 05-26-2008).] IP: Logged |
rnelson
Member
|
posted 05-26-2008 09:23 AM
Thanks Bob for bringing this back on point. quote:
Are countermeasures being employed? If we come to a decision that countermeaures are being used, what studies (if any) can be utilized to support that decision (absent an outright blatant admission by the examinee)? If the data is physiologically or medically ‘abnormal’ (excluding a medical cause), then it must be intentional- and if it is intentional, then it must be a countermeasure?
What is the difference between a strategic plan to alter the test result, and odd/uninterpretable data resulting from a possibly truthful person who may be trying to hard to control his physiological response? Settling the countermeasure question is not as simple as 'yes' or 'no.' Its really a question of whether the data are interpretable or not interpretable, regardless of whether intentional or unintentional. The intentionality of the effort is a secondary concern, and includes things like motivation. Intentionality may be an overly-psychologized approach to this concern, because every truthful person who sits still during a polygraph does so intentionally. For the purpose of discussion, lets assume that we're interested in a "test" in which we know how to interpret the results regardless of a confession or admission. If we think the data are uninterpretable, we then have to ask why that is the case. Do we have enough data to achieve stable measurements/estimates? Some things are obvious, like activity in the movement sensor at CQ9 on Cht 1, correlated with the activity in the pneumos on the same question, and the volcanic EDA reaction. Other things are not so clear. The abdominal activity at CQ4 and CQ6 (cht 1) are present at RQ7 and RQ 10 on the smame chart. You also see this abdominal acivity at CQs, RQs and Ns throughout the subsequent charts. There is mvt activity at RQ7 on chart 2, along with diverging pneumos and a strong EDA reaction. You indicated the subject has had numerous previous polygraphs, but this hardly seem non-naive. I thought Barland had "law of inequality," in which he assumes that strong reactions to RQs are assumed to be valid. There is additional desynchronization of pneumos at RQ10 on chart 2, and then blocking at answer on RQ5 on cht 3. The question for us is: would a CM savvy subject produce these data? Mathematically, the question is: do the artifacts seem to occur randomnly or non-randomly. OSS-3 includes policies and equations to address these concerns. First there must be a sufficient volume of interpretable data - at least three charts, for which at least two presentations of each RQ must be interpretable. Interpretable RQs are defined by the condition that there are useable (non-zero/non-artifacted/non-missing) measurements from at least two component sensors. Second, there is a test of proportions, which evaluates the statistical significance of the difference in the locations of artifacts, against that which would be expected if they occurred randomly (accidentally or unintentionally). The real goal of the polygraph is not to determine countermeasures, but to determine truthfulness or deception, despite the fact that we now have to assume almost anyone may be a non-naive subject. All truthful persons will attempt to calm themselves. All deceptive persons have access to CM information, and some truthful persons will attempt to augment their scores. Is it also possible that some truthful persons may feel threatened or challenged by the RQs? Can CQs overcome that? quote:
On your ‘aside note’ Ray “ all motivation theories falls into three categories 1) jack-ass, 2) marine corps, and 3) godfather”; I presume you are referring to the Corps motivational theory of ‘kicking your ass’?
Not exactly. The jack-ass theory of motivation is behaviorism. Rewards and consequences. Carrot-in-front/stick-behind. It's the most over-utilized form of motivational theory. The Marine-Corp theory of motivation is about self-concept and identity. Marines and other soldiers do dangerous and important things, not because of the rewards or potential consequences, but because of who they are, what they are committed to, and what they believe. Its the same reason parents of newborns function for day at a time with only a few hours of sleep - its gotta be done, and its their role to do it. Godfather motivation is about loyalty (usually family). Remember this: quote:
Fredo, you're my older brother, and I love you. But don't ever take sides with anyone against the Family again. Ever.
When people are really stuck in denial, its usually about family loyalty. Children will sacrifice their own well being for their families. In Denver, we have a case withing the last year, in which a 6 year old girl jumped in front of someone shooting at her mother. So why can't this guy pass a sex history polygraph? Maybe he'll loose his family if he tells the whole story. It sounds like he has some contact with them already. To him its just rewards and consequences. If he has the support and contact of his family now, he stands to lose that if he has assaulted other children and tells about it. Earning a holiday pass is trivial. His goal will be to chip away at the professionals confidence in the polygraph. My own scorched-earth solution would be to stop-the-world, and time-out all contact with the family (telephone, email, carrier-pigeon, smoke-signal and everything). That way he has nothing else to lose by telling, and can perceive that he actually has something to gain.
.02
r
------------------
"Gentlemen, you can't fight in here. This is the war room."
--(Stanley Kubrick/Peter Sellers - Dr. Strangelove, 1964)
IP: Logged |
Poly761
Member
|
posted 05-26-2008 10:46 AM
I'll start with some observations/questions regarding C1A, C4 -The upper and lower pneumos present two very dissimilar patterns at C4. There is a decrease in volume of the upper pneumo with an increase in volume of the lower pneumo which also has a noticeable change in the baseline. How is this explained? This pattern can also be seen at C6. As to R5 at C1A I zeroed out the pneumo, zero for the GSA due to the late response at C4 and equal response R5-C6. No significant changes observed in the cardio, comparison(s) to relevant. (0) C1A, R5. END.....
IP: Logged |
Poly761
Member
|
posted 05-26-2008 03:02 PM
C2A & 2B for R5 = +1
C3A & 3B for R5 = 0
C4A & 4B for R5 = 0Which test technique did you run? For all charts I score R5 a "0." Although I am concerned about the differences previsously described in the upper and lower pneumos, I don't see anything that caused me a concern regarding countermeasures (CM). Controlled/deep breathing was observed in C2A and as a consequence it was necessary to zero out the pneumo and cardio. END..... IP: Logged |
Barry C
Member
|
posted 05-26-2008 04:37 PM
Can you measure the two EDA responses in chart 4a for questions CQ4 and RQ5? It appears if one uses the "bigger is better" rule, you could get two different scores depending on whether the manual or detrended signal was used. What is the detrended filtering, and which is correct? IP: Logged |
Poly761
Member
|
posted 05-26-2008 07:37 PM
I read Bob's comment regarding the "detrended" EDA; this is as much as I'm familiar with this term and the first time I've observed this pattern. I don't know how this is to be considered or applied.The EDA response shows the same relative degree and duration at C4 & R5. The "detrended filtering" response again appears to be similar. Whatever its application it flattened out after R5. What creates this response/pattern, how is it measured and what relevance does it have in scoring the EDA? END..... [This message has been edited by Poly761 (edited 05-26-2008).] IP: Logged |
Barry C
Member
|
posted 05-26-2008 07:50 PM
I measured on my screen, and they're not the same, which is why I brought it up.Stoelting has had a detrending feature for some time. It filters out the slow wave forms so that you can better see the reactions, but it shouldn't change scoring (perhaps on average). It is a step up from Lafayette's auto verses manual that they used to use. (I once scored some charts that resulted in scores on the opposite sides of zero depending on whether the EDA was viewed in auto or manual.) This looks like, for the most part, slow drops (and you'll notice the non-detrended is constantly dropping) are filtered and put on a baseline. In any event, I'm curious as to what it's doing. (I have a Lafayette, but I only used it a couple times since the new detrend feature was added. It looks like a much better EDA than they had previously, but this jumped out at me.) IP: Logged |
Poly761
Member
|
posted 05-26-2008 10:04 PM
On my Lafayette (ink) EDA, I measure the 5-8 seconds on the charts prior to question onset as the time frame to begin measuring a response. Are you using the start/stop of a question to measure initial question response, i.e., the grey area on the computerized charts? I don't know about "detrending," but with the very little I have read so far I can't see its value. It simply seems to create more confusion on the charts if it (isn't) to be used for analysis. I almost always run my EDA on manual to record all possible changes. I don't recall having a problem viewing EDA patterns
and it was mostly after repeated manual centering up/down that I would switch to auto. I would consider changing my sensitivity level to compensate for the continual dropping of the EDA pattern. I'll contact Lafayette tomorrow to learn if they have literature on this "detrend" feature. END..... IP: Logged |
Poly761
Member
|
posted 05-26-2008 11:01 PM
Bob -In reference to R7. Did something occur on 4B (question not completed); or is this question repeated on 4C as part of the technique you used? Quite a difference between abdominal/thoracic pneumo reponses for R7 on(4C). Hoping to learn an explanation for these unusual pneumo differences. I understand the countermeasure concerns. But, try to record a similar pattern on your instrument. Average breathing on either abdominal or thoracic and a steady increase in volume on the opposite pneumo of four cycles or more. What am I missing? END..... [This message has been edited by Poly761 (edited 05-26-2008).] IP: Logged |
rnelson
Member
|
posted 05-26-2008 11:57 PM
quote:
Quite a difference between abdominal/thoracic pneumo reponses for R7 on(4C). Hoping to learn an explanation for these unusual pneumo differences.
simple: undercooked roast beef and boiled cabbage for lunch... It seems possible to me that the pattern at R7 is not the result of a respiratory CM, but voluntary muscle activity being recorded through the pneumo sensor. The descending lower tracing is the result of a contracting sensor. Is it possible that could that occur if an examinee attempts to freeze or hold his abdominal activity still at the point of answer? He's obviously trying too hard, and its working against him. I believe it is possible to get too wrapped up in this. The goal is to separate truthful people from deceptive people. A problem is that the signals are noisy to begin with, and that is compounded by the fact that both truthful and deceptive people do things in hope to "pass." We are still primarily concerned about the data points that most effectively separate truthful people from deceptive people. The challenge is to not be misled by data that is uninterpretable, meaningless, or adultered. These pneumos stink. Is he trying too hard? Probably. The real question is whether or not we conclude he is deceptive. Are the remaining interpretable data sufficient to reach a reliable and valid conclusion on that? To ask it differently, do we think the EDA and cardio data/reaction-segments are secondary to or caused by the voluntary activity recorded in the pneumos? r ------------------
"Gentlemen, you can't fight in here. This is the war room."
--(Stanley Kubrick/Peter Sellers - Dr. Strangelove, 1964)
IP: Logged |
Poly761
Member
|
posted 05-27-2008 09:36 AM
I believe the pneumos present good clear tracings. My continuing concern, not conclusively explained, are the differing pneumo cycles at the same question(s) we are discussing. I used the identified "4-cycle staircase pattern" as an indices for many years. How can we accomplish " - our goal to separate truthful people from deceptive people" if these cycles can't be explained. I don't recall observing these patterns occurring simultaneously at one question. It's almost like the pneumos are attached to two separate persons. Although it doesn't appear these pneumo patterns impact the other components I wouldn't render a conclusive opinion at this time without being able to explain (why) this is occurring. Which of the two pneumo patterns do you use for analysis if we can't conclusively explain why we would use one over the other? END..... IP: Logged |
stat
Member
|
posted 05-27-2008 11:55 AM
ah pneumos-------the ball and chain of polygraph.I see the pneumos as being like the rolling credits of a movie----they're useless and ignored 90% of the time unless you have a specific correlative interest i.e. was that filmed in Alaska or Canada? Are we seperating fly shit from pepper here? It's all a bunch of noisey data, and if an examiner can really get past the artifacts and see truth or lie, than I need to study with such a master. [This message has been edited by stat (edited 05-27-2008).] IP: Logged |
Poly761
Member
|
posted 05-28-2008 02:37 PM
Stat -What are defining as "noisey data?" END.....
IP: Logged |
Barry C
Member
|
posted 05-28-2008 03:25 PM
Okay, I scored the first three charts just for kicks:I have a DI score based on a spot score of -7 for RQ7. Personally, I don't mind calling a chart with distorted tracings DI. I wouldn't call it NDI. Some may not like that, but it goes back to polygraph in its purest form, so to speak. We have consistent, significant reactions to at least one of the RQs - despite the person's apparent attempt to make a mess of things. I would have little to no confidence in a NDI decision if scoring were to have resulted in positive scores above the requisite cut-off. There is a possibility that an (Truthful) examinee could have bought into the CM crowd's "need to manipulate to pass" baloney, but I would expect to hear about that in the post-test interview when they learn they were lied to by GM. IP: Logged |
stat
Member
|
posted 05-28-2008 07:24 PM
Poly761,Although an unoriginal label for the pneumos, "data noise" is a referance to all the loop-de-loops and eye catching irregularities that we don't have any good answers for. Really, some of the theorizing for just what is going on is pretty reaching. example;
I believe we are seeing a person with a hernia who has sore surrounding muscles from doing a roofing job the day before---and that he is controling his breathing in addition to the pain.
Of course there are many much smarter people than me who hold on to the validity of pnuemographic data other than to look at gsr contaminates. I get it. That doesn't make chart interpretation with what looks like a reptile's breathing patterns any easier or compelling to detracters. Benussi would be proud of some of you.
IP: Logged |
Poly761
Member
|
posted 05-28-2008 11:42 PM
I can't account for the previously identified pneumo patterns that I haven't experienced in the past and (to me)are unusual. I don't know the exam technique used. It doesn't appear R7 question was asked in full on Chart 4B and repeated on 4C. Answers to these questions likely affect scoring. I will render a conclusive opinion on charts with distorted tracings as long as the distortions didn't impact on the indices being evaluated. I'd call these charts INC, conduct a strong post test interview and then conduct a single issue UTAH. END..... IP: Logged |
Bob
Member
|
posted 05-29-2008 08:32 AM
Sorry I haven't commented on this lately- will try do to do so later this evening. Have just gone through some dental work and I'm a mess.Bob IP: Logged |
rnelson
Member
|
posted 05-29-2008 10:53 AM
Sounds like serious dental work Bob. We're all looking forward to the rest of the story.I believe the technique is a plain-'ole Zone or Zone variant. The CQs are rotated. The aborted/repeated RQ7 is on the 4th chart, so I don't think that affects much. Even so, repeating a question is allowed, and this one was preceded by a neutral question. It might have been better to do a repeat a CQ after the neutral, but who knows. I agree the pneumos are odd and should not be trusted. That is what "noisy" means. The signal (normal autonomic respiration and reaction to test stimuli) are contaminated by peripheral/somatic activity (behavior) that has not much, if anything to do with respiration. Separating the two is, as stat says, like trying to separate pepper from fly specks. Cardio data become noisy too, when we see recurrent PVEs or respiratory blood pressure fluctuation. Under those circumstances is becomes very difficult to separate the signal (blood pressure change) from the noise (spike, or oscillation). EDA data become noisy and difficult to interpret when the data are plunging, and when the data are labile. Look at cht2c (above) and you'll see what looks to me like a problem. The raw EDA on C4 is plunging, while the detrended EDA shows a small ascending segment after answer, of almost 1/2 chart division. The next question, R10 shows both raw EDA and detrended EDA both show an ascending segment shortly after answer, of just over 1/2 chart division. The problem, for me, is that ascending segments are interpreted as indicative of sympathetic activation. The raw EDA at C4 does not indicate sympathetic activation, and what looks like sympathetic activation in the detrended EDA is fictitious - it is a feature of the filter's math, and not the sympathetic nervous system. It seems like I've seen this concern somewhere else, but I cannot recall where. Getting back to the pneumos. The data, from Kircher, et al., Harris, et al, and others, have consistently suggested that properly interpreted pneumo data are additive to decision accuracy, and do not degrade decision accuracy. This is consistent with what we found in training OSS-3. Any suggestion to the contrary should be backed up by data and not just vague allusions to smart people. The key is "properly interpreted." The general trend in the science of polygraph seems to be a movement towards a measurement based approach to scoring features, and away from a pattern-recognition approach. Anytime we start talking bout measurements, we have be thoughtful about scaling assumptions, and what the data are capable of telling us. Do we measure in mm or inches, and are the data linear or not. In the case of unproven assumptions, we often resort to nonparametric a
IP: Logged |
Poly761
Member
|
posted 05-29-2008 11:42 AM
Good Morning -What was the computer score on these charts? Quote:
"I agree the pneumos are odd and should not be trusted. That is what "noisy" means. The signal (normal autonomic respiration and reaction to test stimuli) are contaminated by peripheral/somatic activity (behavior) that has not much, if anything to do with respiration." If it is agreed the pneumos are odd & can't be trusted, how can a conclusive opinion be rendered? I don't agree the respiration pattern in question is the result of somatic activity. The pattern is too clear, consistent and well defined as is expected in the "average" respiratory pattern. I'd like to see what patterns this examinee produces when sitting undisturbed by questions. END..... [This message has been edited by Poly761 (edited 05-29-2008).] IP: Logged |
rnelson
Member
|
posted 05-29-2008 04:02 PM
quote:
If it is agreed the pneumos are odd & can't be trusted, how can a conclusive opinion be rendered?I don't agree the respiration pattern in question is the result of somatic activity. The pattern is too clear, consistent and well defined as is expected in the "average" respiratory pattern. I'd like to see what patterns this examinee produces when sitting undisturbed by questions.
Good questions. The answer is to think about what we me when we say "conclusive." What we seem to mean is "not inconclusive." It is important again not to take the language itself too literally. All tests are math tests (even spelling tests), and all test results are simplified probability statements. When scoring at test with data of compromised interpretable quality, the question become one of whether the remaining data are of sufficient interpretable quality to render a decision that provides adequate reliability (would others agree), and validity (does it mean what we say it means). When scoring a polygraph test, the practical meaning of the test results is different for DI and NDI exams, and that will change based on the testing circumstances (e.g., LEPET screening exams compared to an investigation of a spouse who is missing under suspicious circumstances). There is nothing wrong with being conservative about the interpretability of polygraph data, but it accomplishes little to create artificial dichotomies in which we either pretend that everything is usable, or else discard everything. I'll re-iterate that the trend has been to move away from pattern recognition and toward measurement, even ordinal measurement, in TDA. So here are the pattern. Cht2a
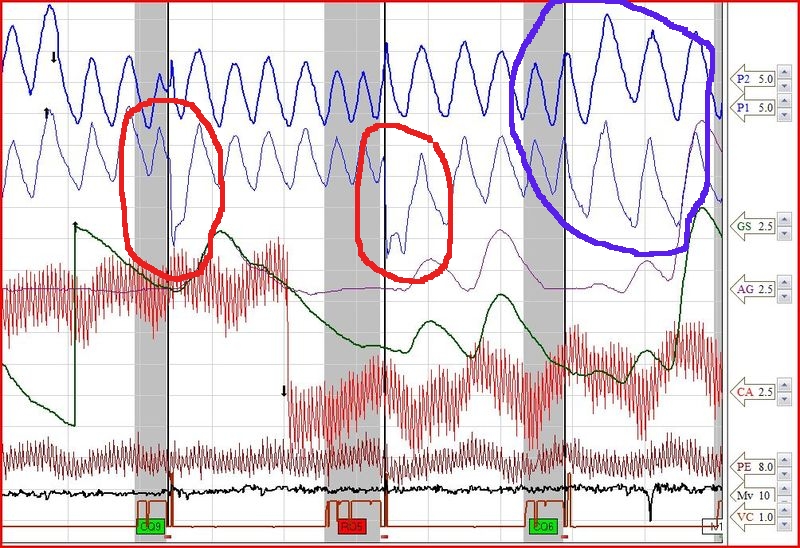 I've circled a couple of the lower pneumo features in red. We might be looking at different things. Are you suggesting this pattern, the result of a contracting lower pneumo sensor, is autonomic (not somatic)? Also, note the diverging upper in lower pneumos (circled in blue). It seems to me that it would take quite a bit of behavioral effort to make the sensors produce this data. 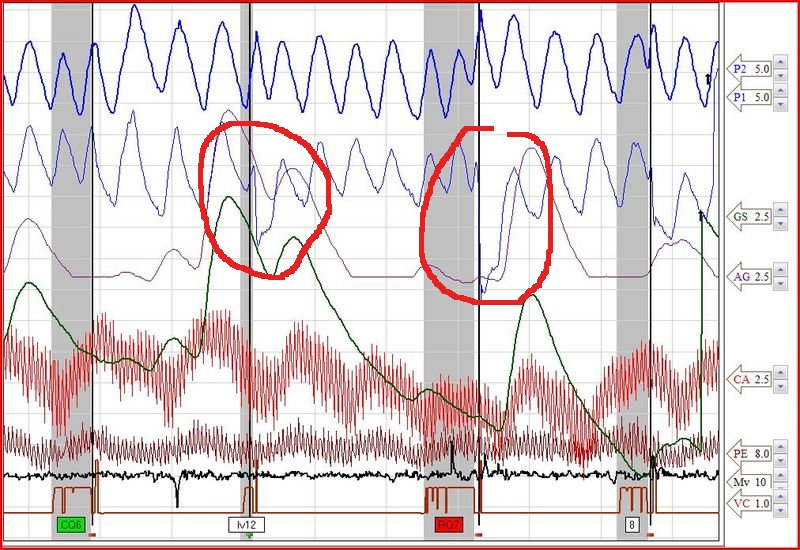
The lower pneumo patter occurs throughout the exam, at CQs, RQs and Neutrals. It seems rather dumb to attack the RQs like that. 
It may not be convincing to suggest this guy has a well defined strategy. However, our choices in interpreting these data are 1) autonomic production of these data, or 2) somatic activity. I'll go with door #2.
.02
r
------------------
"Gentlemen, you can't fight in here. This is the war room."
--(Stanley Kubrick/Peter Sellers - Dr. Strangelove, 1964)
IP: Logged |
Poly761
Member
|
posted 05-29-2008 05:33 PM
It appears we are looking at and referencing different responses on the charts. I'll address your comments first.I agree, the responses you have circled appear in almost every question. Look at where they occur. In almost all questions they occur, to one degree or another, at the time the question is answered. This is what I was instructed to define as an "answering mechanism," (old term). In this test, in my opinion, what you are circling in red is an overexagerated response to a question on the exhalation cycle. Likely a deliberate attempt to distort the patterns (which did occur). What you have circled in blue, in my opinion, is a change in the rhythm, volume and regularity of the respiratory pattern. Deliberate changes/distortions. Is the downward spike at the bottom of the chart at CQ6 an indication of movement? The pneumo changes I have been referring to begin on Chart 1B, CQ6. You've already seen CQ6 and RQ7 on 1B have the same exagerated response pattern at the point the question is answered. The changes I question are the 4 respiration cycles recorded by the lower pneumos, beginning immediately after the distorted answer to CQ6 & RQ7. Compare these to the upper pneumos recorded at the same time. The upper pneumos are recording a relatively "average" pattern while the inhalation/exhalation cycle of the lower pneumos is slightly changing at the same time, a suppressed pattern. What are your thoughts? END..... [This message has been edited by Poly761 (edited 05-29-2008).] IP: Logged |
Poly761
Member
|
posted 05-31-2008 09:06 AM
Bob -I hope you're feeling better. Do you have any objection if I copy some or all of your charts for review with other examiners? I still have some unanswered questions and I believe they are great charts for discussion. END..... IP: Logged |
Barry C
Member
|
posted 05-31-2008 09:42 AM
A silent answer test is a nice way to get rid of those answer distortions. When a person answers a question at the end of an exhalation, then of course you are going to see a drop in the tracing. (These are very dramatic, I agree.)I seem to recall a Kircher(?) study in which they "smoothed" out answer distortions (some type of editing) to avoid measuring (and therefore scoring) them (with the computer). The results were good, meaning we are probably safe to ignore answer distortions when we score by hand. (I'm afraid to say that as I know some could take that too far.) It's just one more thing to consider. IP: Logged |
rnelson
Member
|
posted 05-31-2008 11:51 AM
Poly761,Thanks for clarifying. The answering artifacts seem to me to be excessive. They are sometimes seconds in duration. That's kind of a long time. Barry, Kircher & Raskin (1988) described interpolating artifacts that were 1 to 3 seconds in duration. They also described using a step-wise averaging procedure (probably analogous to a low-pass filter) to smooth the EDA, and smoothing answering artifacts for 2 samples (1 second) preceding and following the answer. Here is an example of 40 seconds of Pneumo data 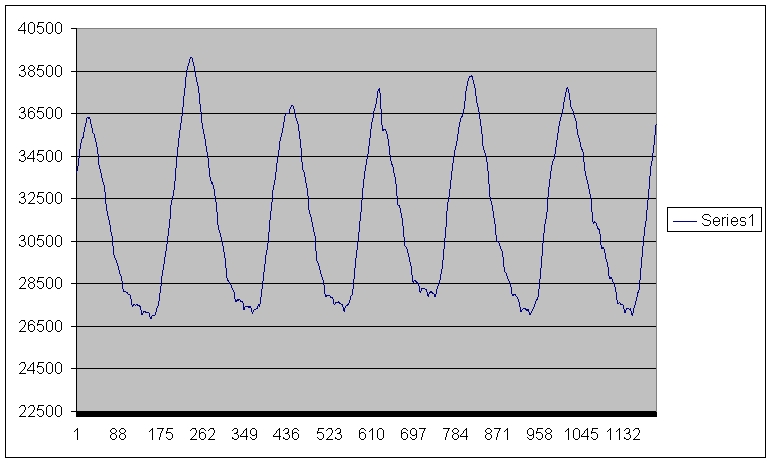 You can see imagine that high-frequency noise at the bottom of the respiratory cycles will distort the accuracy of a linear measurement of respiratory excursion (RLL). You can see imagine that high-frequency noise at the bottom of the respiratory cycles will distort the accuracy of a linear measurement of respiratory excursion (RLL).
The point is that some filter is appropriate, and may improve the accuracy of our measurements. Below is the same data smoothed with a .5 second step-wise procedure.
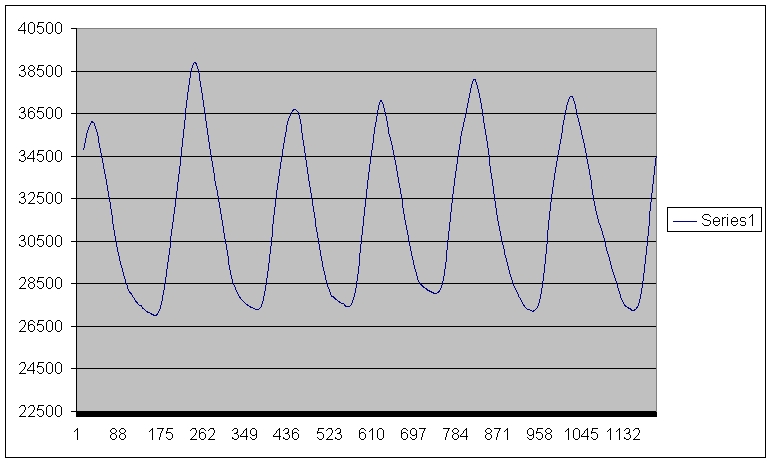 More filtering isn't always better. The same data, below, are smoothed to a 2 second step-wise interval. Look familiar? More filtering isn't always better. The same data, below, are smoothed to a 2 second step-wise interval. Look familiar? 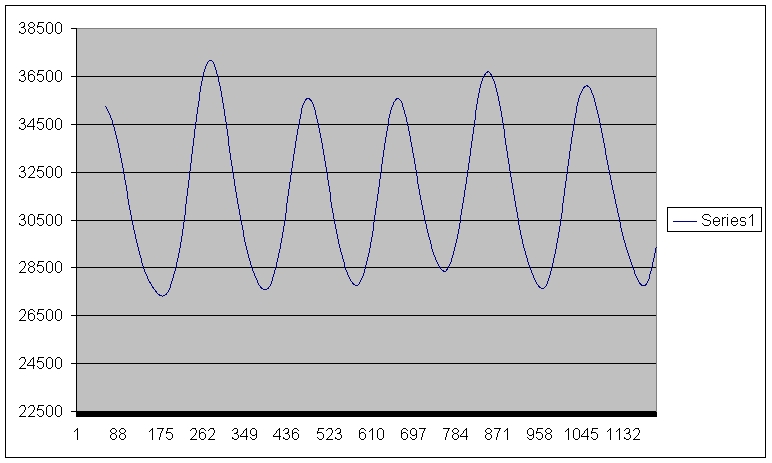
r
------------------
"Gentlemen, you can't fight in here. This is the war room."
--(Stanley Kubrick/Peter Sellers - Dr. Strangelove, 1964)
IP: Logged |
Barry C
Member
|
posted 05-31-2008 05:51 PM
Interesting... and yes, it does look familiar, but I'm biting my tongue.IP: Logged |
Bob
Member
|
posted 06-02-2008 08:52 PM
Good Evening Everyone- I apologize for the delay in my follow-up posting (had to undergo some dental surgery and just haven’t been in right frame of mind lately). The Rest of the Story is at the end of the post, but to address some of your questions: The format being utilized was the Army Modified Zone Comparison Test (AMZCT) with emphasis on Sex Hx screening regarding unreported child victims. As you will see later in this posting- my scores are different. To jump ahead of myself, I scored DI to RQ 7 (-4/-5), but positive scores to RQ 5 and 10 (score sheets are at the end of the post). Others on the Forum who took the time to evaluate the charts (Ray, FedEmployee, and Barry), are reporting DI to RQ 7 as well; Poly761 ended with Inconclusive. However, I ultimately rendered an Inconclusive decision. Poly761 asked if something happened at R7 on Cht 4b, and the answer is ‘yes’, I started the question off wrong-and stopped before completion of the question and immediately told him the question would be repeated- he gave no verbal response. Ray: you commented C6 is too early to use on Cht 1 and there is movement at C9, making R10 unscoreable: I would agree with you that C6 cardio and EDR are too early for comparative purposes, although the pneumo is of ‘?value?’. I disagree with R10 being unscoreable due to C9 movement. True there is some minor movement occurring at C9 (but bear in mind the Mov Sens is set at SU 10), and in my opinion the movement is minor and did not cause the initial cardio arousal, and certainly did not cause the secondary cardio response. The pneumo rate change with suppression at C9 however is occurring early. Fed Employee: commented My issue is the pneumos- inconsistant. Attempted countermeasures?[/]; and Fed this is the reason for my submitting the polygrams. The subject presented himself as being very cooperative, however I highly ‘suspect’ a low level of countermeasures being utilized via general covert disruptive behavior in an effort to preempt test data analysis. Bill2E: you wrote [i]It appears there are breathing countermeasures, however this could be due to the medications I would disagree with the medications as being the ‘cause’ for the abdominal baseline shift with apnea. We can see in the charts there was no such baseline shifts with apnea on other questions posed. Refer to Cht 1c-1 above. Poly761 asked how is this explained (referring to the pneumo desynchronization) but adds the pneumos did not cause him concern regarding countermeasures What I believe is occurring is the subject is deliberately ‘switching’ at times to contracting the abdominal muscles, and holding that contraction, at the moment he inhales in the thorax with no air trapping occurring (inhibition) at times. Look at the following two chart segments:
 Ray also commented on this it seems possible to me that the pattern at R7 in not the result of a respiratory countermeasure, but voluntary muscle activity being recorded....it is possible that could occur if an examinee attempts to freeze of hold his abdominal activity still at the point of anwer Which I agree on the mechanics, but I see it as being ‘abnormal physiology’ and that he is doing so voluntarily (therefore deliberately) to create ‘something different’ - the countermeasure. Take a look at the following chart re-creation attempts: 
 Ray earlier posed ...The real goal of the polygraph is not to determine countermeasures, but determine truthfulness or deception....all truthful persons will attempt to calm themselves. All deceptive person have access to countermeasure information, and some truthful persons will attempt to augment their scores...I believe it is possible to get too wrapped up in this. The goal is to separate the truthful from the deceptive I agree with you, Ray, the goal is to separate the truthful from the deceptive- but if the person is being grossly disruptive (or covertly disruptive while merely trying to give the pretense of cooperation) or engaging in ‘sophisticated (learned) countermeaures- why would we want to report him as being ‘truthful’ or ‘deceptive’- particularly Truthful? So therefore we must assess the use of countermeasures(including disruptive behavior by deliberately inducing abnormal physiology)-I would say “garbage data in- garbage decision making out.” AND THE REST OF THE STORY: Below are my numerical score sheets- no doubt we will have some disagreement here as I'm not that confident two examiners always agree entirely. I hope my score sheet and notations are not too confusing (I tried to give some side explanations). Polyscore v6 was No Deception Ind. (Spot Scores R7- .86; R5-.77; R10-.06).
Although I numerically scored R7 as -4/-7; notice however the same question using respiratory RLL measurements went totally in the opposite direction with R7 as +4/+5; as stated above Polyscore v6 was indicating No Deception also. I then considered the pneumos, being so ‘physiologically abnormal’ that in my opinion with ‘more than likely countermeasures being utilized, that I made a final decision of Inconclusive. Post Test Interview: The subject states he was being truthful to the questions posed. However he admits he wanted to sabotage the test because he did not want to attend the family holiday gatherings. He said he did not want to attend the family gatherings because he knew there would be children present (nieces-nephews) and felt assured he would begin to visualize them nude and sexually fantasize about them. He did not want to tell his family the reason for not wanting to attend, but wanted to say ‘his therapist’ would not allow it; thereby shifting the blame to the therapist; and at the same time he could avoid telling the therapist the real reason ‘why’ he didn’t want to attend by shifting the blame to the polygrapher by saying “I’m just so nervous I can’t pass a polygraph”. Although he admits he wanted to sabotage the test, I could not get him to fully and completely explain to my satisfaction ‘just exactly how’ he tried to accomplish the task. So Ray, you are not too far off with your statement ...Maybe he will loose his family if he tells the whole story....his goal will be to chip away at the professionals confidence in polygraph....
 
sorry for all the edits-trying to resize the score sheet so it's readable. Bob [This message has been edited by Bob (edited 06-02-2008).] [This message has been edited by Bob (edited 06-02-2008).] [This message has been edited by Bob (edited 06-02-2008).] [This message has been edited by Bob (edited 06-02-2008).] [This message has been edited by Bob (edited 06-02-2008).] [This message has been edited by Bob (edited 06-02-2008).] [This message has been edited by Bob (edited 06-02-2008).] [This message has been edited by Bob (edited 06-02-2008).] IP: Logged |
rnelson
Member
|
posted 06-03-2008 12:46 AM
Bob,That was thorough and highly instructive. Great job. Excellent markup on the charts too. I've seen that lower pneumo pattern before and suspected it was muscular activity. Thanks for the time and effort to dissect, replicate it, and tell us about this interesting case.
r
------------------
"Gentlemen, you can't fight in here. This is the war room."
--(Stanley Kubrick/Peter Sellers - Dr. Strangelove, 1964)
IP: Logged |
stat
Member
|
posted 06-03-2008 08:30 PM
Bob Weeks----a cautious, steely-eyed examiner with eyes on the future. Bob, you are a credit to the field. Of course, you are also a fellow Hoosier. Nice presentation of hard work and transparency of methods.Inexperienced examiners must see ugly field charts to understand better the challenges of deciphering how to call such ugliness. I'm reminded of how Joe McCarthy has endlessly boasted of his inability to have inconclusives. It just shows his ignorance. We see plenty of nasty charts in the field, and in my anecdotal experience, the smokeiness nearly always originates from those GD pneumos (!). IP: Logged | |


 Polygraph Place Bulletin Board
Polygraph Place Bulletin Board



